An anal fistula is a common condition that causes pain, skin irritation, and foul-smelling pus.
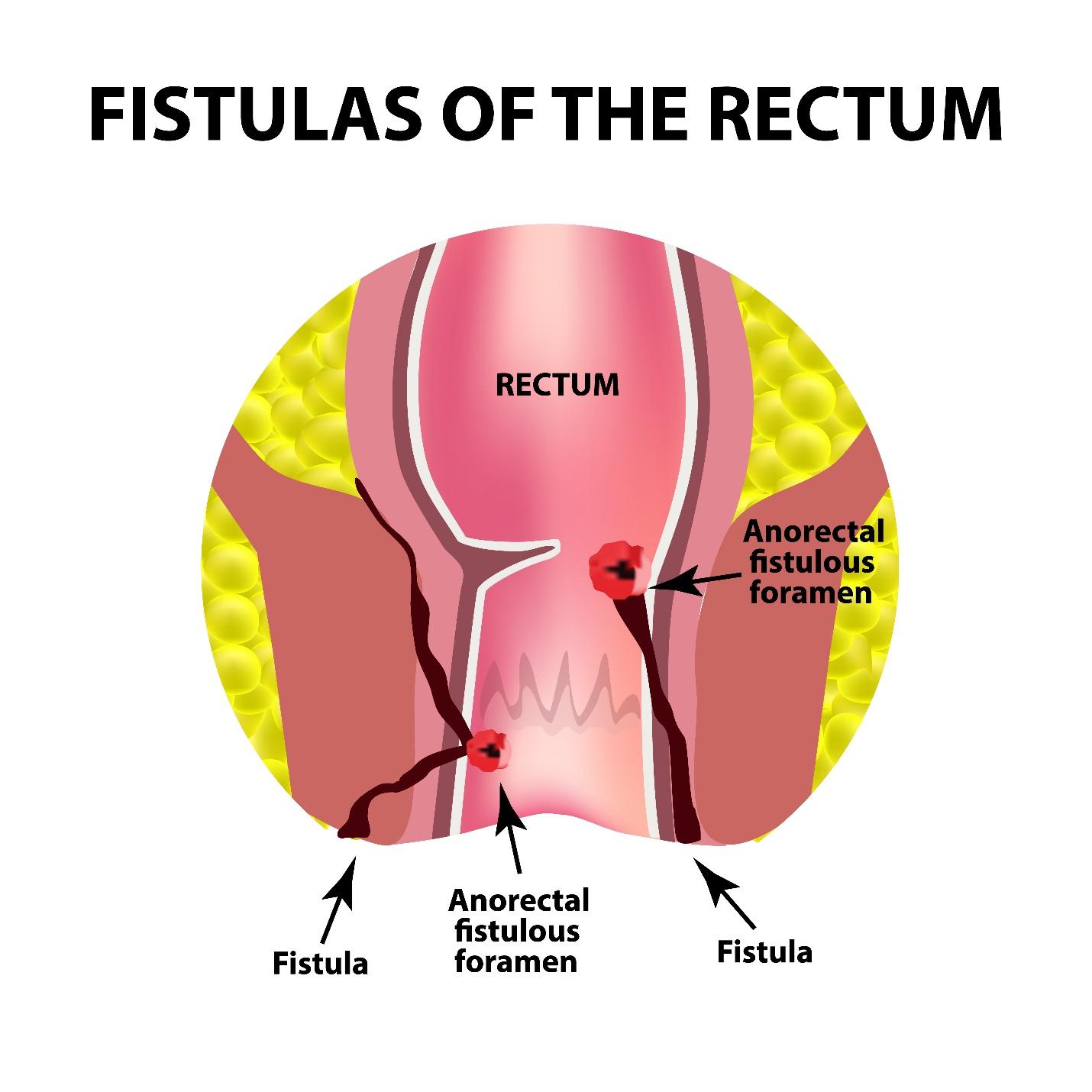
An anal fistula is an abnormal tunnel that forms between the anal canal, and the skin around the anus. It usually develops after an anal abscess, a pocket of pus, drains on its own or is surgically treated, leaving a tract behind. This condition can cause chronic pain, persistent discharge, and recurring infections if left untreated. Although anal fistulas are not life-threatening, they require medical attention to prevent complications.
What are the different types of Anal Fistulas?
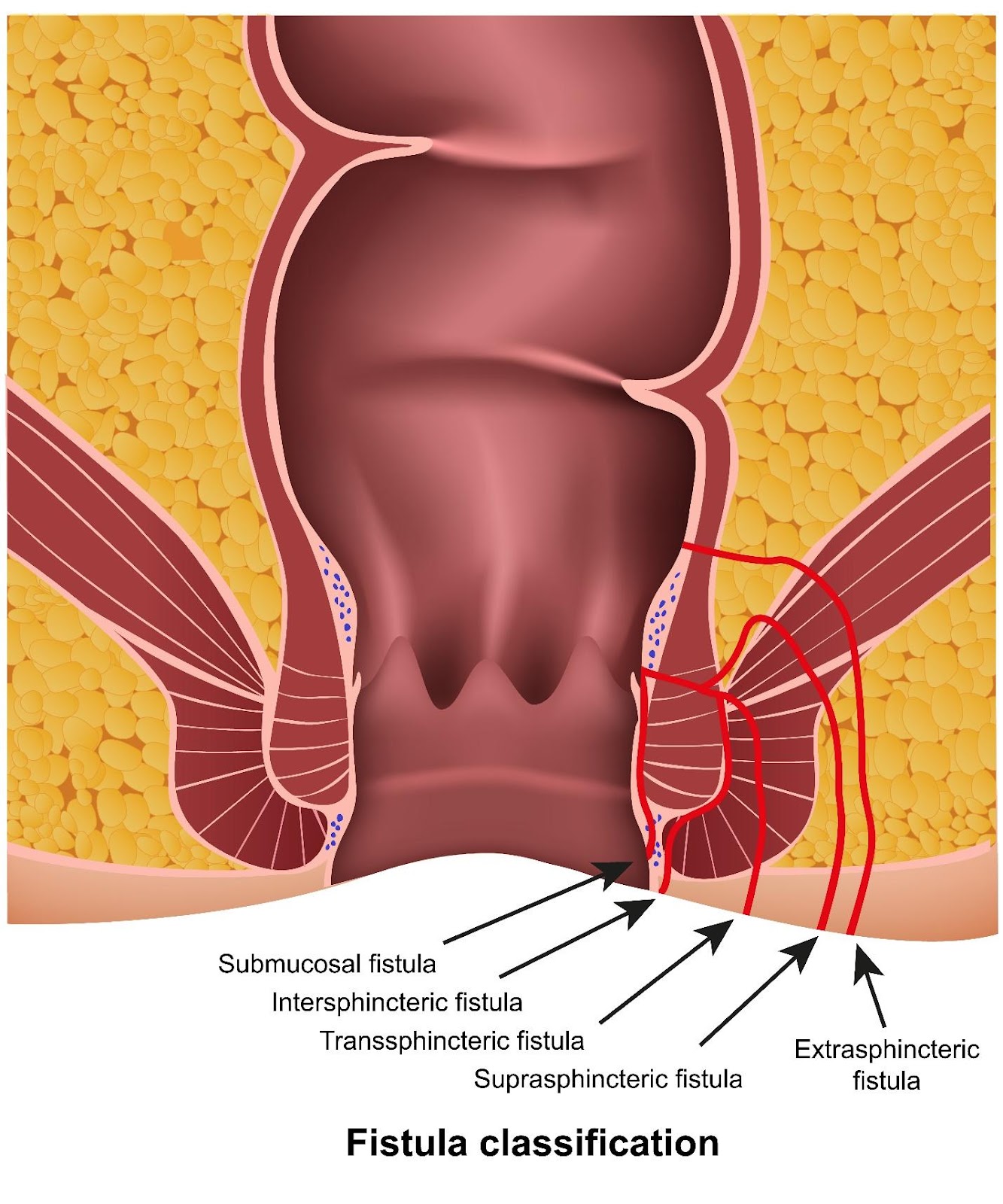
Anal fistulas can be classified based on their pathway and relation to the anal sphincter muscles:
Intersphincteric Fistula– the tract runs between the internal, and external sphincter muscles.
Transsphincteric Fistula– the tract crosses through both sphincter muscles, making treatment more complex.
Supralevator Fistula– the tract loops above the external sphincter and is rare. The causes include an underlying disease like Crohn's disease or a traumatic event such as an embedded bone
What causes an Anal Fistula?
The most common cause of anal fistulas is a previously untreated or improperly healed anal abscess. However, several other factors can contribute to their development:
Anal abscess– when an infection occurs in the anal glands, it can lead to an abscess. If this pocket of pus fails to heal completely, it may develop into a fistula.
Cancer – although rare, certain, anal cancers can cause or mimic anal fistulas.
Crohn’s disease–Inflammatory bowel diseases (IBD) like Crohn’s can trigger chronic inflammation in the digestive tract, including the anus, increasing the risk of fistulas.
Infections – Sexually transmitted infections (STIs), and tuberculosis affecting the anal region can occasionally result in fistulas.
Radiation therapy – in some cases, patients undergoing radiotherapy to the pelvic region may develop, anal fistulas as a side effect.
Trauma or Surgery– previous anal surgeries or injuries to the anal area may also create conditions for fistula formation.
What are the symptoms of an Anal Fistula?
Anal fistulas are classified based on the location that it is formed.
The symptoms of anal fistulas vary depending on the location, and severity, but common signs include:
A foul-smelling discharge that may stain underwear.
Pain, especially when sitting or during bowel movements.
Persistent pus or bloody discharge from an opening near the anus.
Recurring abscesses in the same location.
Skin irritation or swelling around the anus.
Occasionally, fever if an active infection is present.
Who is at risk of developing Anal Fistula?
Although anal fistulas can occur in anyone, certain groups of people are at a higher risk due to specific health, lifestyle, and medical factors. These include:
Crohn’s disease – people with IBD, particularly Crohn’s disease, face a much higher risk of fistula formation due to chronic inflammation, and ulceration within the intestinal tract and anal region.
History of anal abscesses – individuals who have experienced recurrent anal abscesses are at a significantly higher risk of developing an anal fistula, especially if the abscesses were inadequately treated or repeatedly infected.
People with compromised immunity – individuals with weakened immune systems, such as those with diabetes, HIV or chronic infections, may be more vulnerable to persistent infections that can progress into fistulas.
Prior pelvic radiation therapy – patients who received radiation therapy to treat cancers in the pelvis or lower abdomen may develop radiation-induced tissue damage, increasing the risk of fistula formation.
How is an Anal Fistula diagnosed?
Diagnosing anal fistula involves a comprehensive assessment to confirm its presence, map its tract, and identify potential underlying causes. Here at Alpine Surgical Practice, a consultation generally includes:
Medical history and physical examination
Medical history review – our doctor will assess your symptoms, past medical history, and any history of anal abscesses, surgery or IBD.
Physical examination – a thorough examination of the anal region will be conducted. This includes inspecting for any visible external openings, discharge or tenderness around the anus.
Additional Diagnostic Tests
Colonoscopy – if IBD, like Crohn’s disease, is suspected, our doctor may recommend a colonoscopy to examine the entire colon, and rectum.
Fistulography – this imaging test may involve injecting a contrast dye into the external opening, followed by X-rays to outline the full extent of the fistula tract. This is now rarely performed
Magnetic Resonance Imaging (MRI) – for complex or recurrent fistulas, an MRI provides detailed imaging of the fistula tract, its relation to the sphincter muscles, and any associated abscesses.
What are the treatment options for Anal Fistula?
Once doctors have confirmed a diagnosis, and the type of fistula, they will proceed to outline a comprehensive treatment plan.
The treatment approach for anal fistulas is determined by factors such as the fistula’s complexity, its proximity to the anal sphincter muscles, and the presence of any underlying medical conditions. Treatments for anal fistula can include:
InitialTreatments
Initial treatments aim to tide over the acute event to offer the patient pain relief and to serve as a bridge to eventual surgical treatment:
Abscess drainage – if an associated abscess is present, our doctor will perform incision, and drainage to relieve symptoms.
Antibiotics – when infection is present, antibiotics can manage the infection, although they do not cure the fistula itself. Antibiotic therapy serves to tide over the acute infection till definite surgical treatment can be performed
Pain management – medications such as analgesics may be prescribed to relieve discomfort.
Surgical Treatments
In some cases, definitive treatment for anal fistulas requires surgery. Our doctors offer several innovative surgical options, including:
Advancement flap repair – an advancement flap repair involves using a flap of healthy rectal tissue to cover the internal opening, closing off the fistula.
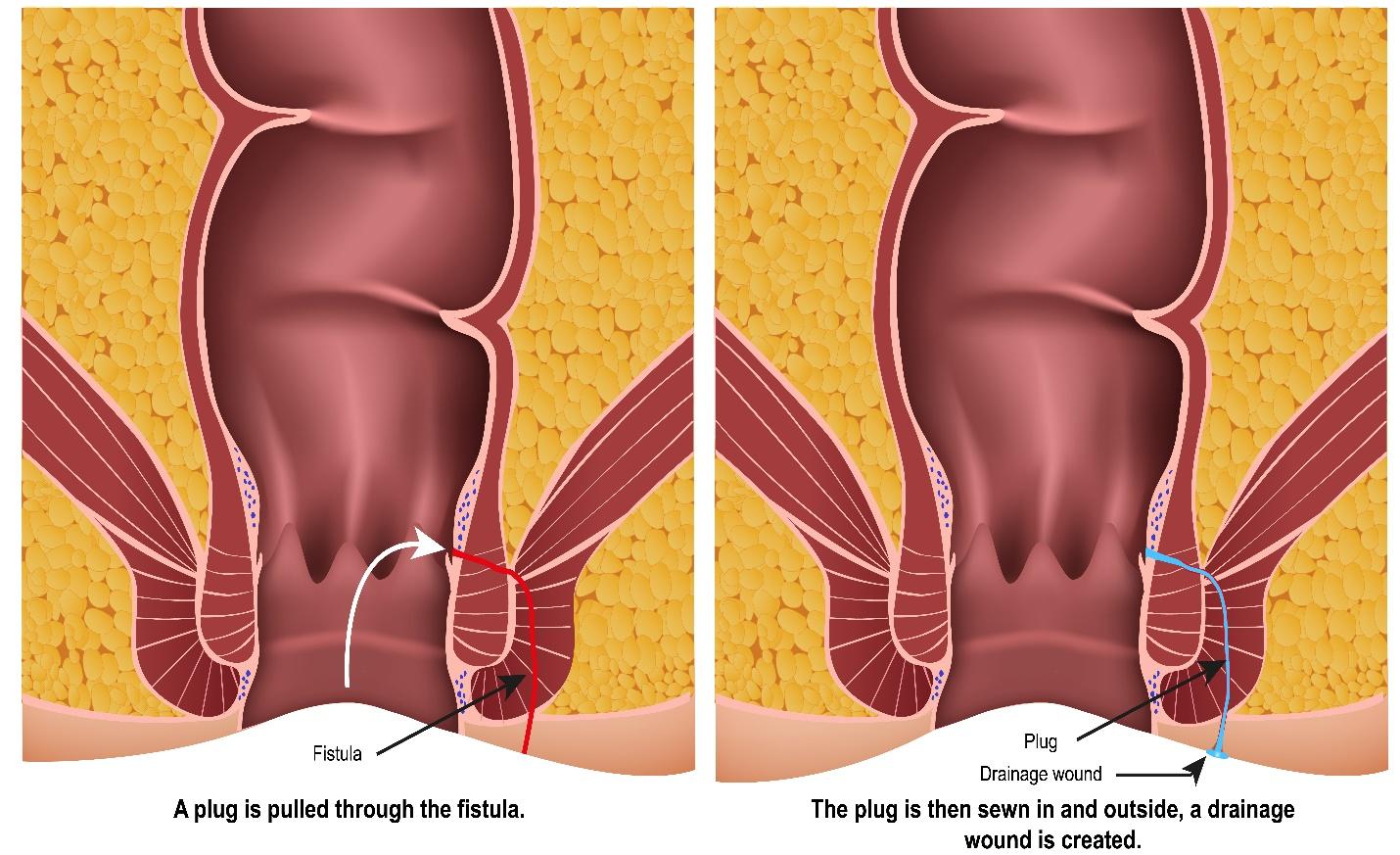
Fibrin glue or plug – in certain cases, the fistula tract can be sealed with fibrin glue or a bioprosthetic plug, encouraging tissue regeneration and closure of the tract.
Fistulotomy – for simple fistulas, the tract is surgically opened, and flattened to heal as a scar. This approach is highly effective for superficial fistulas.
Ligation of Intersphincteric Fistula Tract procedure (LIFT) – this sphincter-preserving technique accesses the tract from a small incision in the perianal skin, allowing the internal opening to be securely ligated, and the tract removed.
Seton placement – for complex or high fistulas involving the sphincter muscles, a seton (surgical thread) is placed to keep the tract open, and allow gradual drainage and healing while preserving sphincter function.
Interposition flap - In highly complex fistula with large tissue defects and non-healing status, an interposition flap (usually a muscle flap) may be employed to close off the defect and bring in fresh tissue to promote healing
Management of Underlying Conditions
In cases where anal fistulas are linked to chronic conditions such as Crohn’s disease, effective treatment goes beyond addressing the fistula itself.
This may involve:
Monitoring disease activity – Regular follow-ups and diagnostic assessment, such as colonoscopy or imaging studies, help monitor the progression of the disease, and detect new fistulas or complications early.
Nutritional support – a balanced diet tailored to the patient’s specific condition can help improve gut health, enhance healing, and reduce flare-ups.
Optimising medications – patients with Crohn’s disease or IBD may need adjustments to their immunosuppressants, biologics or anti-inflammatory medications to control inflammation, and reduce the risk of recurrent fistulas.
Summary
If you have been living with persistent anal pain, discharge or recurring abscesses, know that you do not have to endure this alone and your condition is treatable. Timely diagnosis, and tailored treatment can make a world of difference to your comfort, and well-being. At Alpine Surgical Practice, Dr Aaron Poh offers compassionate, discreet care backed by extensive experience in treating anal fistulas. With evidence-based techniques, and a personalised approach, we are here to help you heal, and regain your quality of life.
What happens if an anal fistula is left untreated?
Leaving an anal fistula untreated can lead to various complications, including:
Underlying serious conditions such as anal cancer could be missed if the fistula is not properly assessed, and treated.
Development of complex, branching fistula tracts that are more difficult to treat.
Potential damage to the anal sphincter muscles, affecting bowel control.
Recurrent infections, and abscess formation.
Can an anal fistula heal without surgery?
Unfortunately, anal fistulas almost never heal on their own. While conservative options may be suitable for the initial treatment, surgery is the definitive treatment for most cases. Delaying treatment allows the fistula to progress, increasing the risk of complications, and more challenging surgeries.
How serious is an anal fistula?
Anal fistulas are not usually life-threatening, but they are a chronic condition that requires medical attention. If it is left untreated, they can result in:
Rarely, the presence of a fistula could obscure or delay the diagnosis of a more serious condition, such as cancer.
Formation of more extensive and difficult-to-treat fistula tracts.
Persistent pain, discharge, and infections.
Can anal fistulas come back after surgery?
While surgical treatment is highly effective, recurrence is possible, especially if the underlying cause, such as Crohn’s disease, is not well managed. However, working with an experienced doctor significantly reduces the risk of recurrence.
How long does recovery take after anal fistula surgery?
Recovery times vary depending on the complexity of the fistula, and the type of procedure performed. In general:
Most patients can resume light activities within 1 to 2 weeks.
Full healing may take several weeks to a few months.
Regular follow-up appointments are essential to monitor healing, and catch any signs of recurrence early.
How can I prevent anal fistulas from recurring?
To lower your risk of recurrence, you can:
Avoid unnecessary trauma to the anal area, including improper use of enemas or anal intercourse without adequate lubrication.
Maintain good anal hygiene.
Seek prompt treatment for any anal abscesses or infections.
Work with our doctor to manage chronic conditions like Crohn’s disease.